O ASAIO Journal publicou um estudo de caso, em inglês, sobre a primeira criança Neonatal a ter sua vida prolongada por meio da ECMO (oxigenação extracorpórea com membrana), em 1975. O artigo conta com os comentários do professor Professor Robert Bartlett e pode ser lido na integra nesta postagem, ou baixado em PDF clicando AQUI.
O artigo também pode ser visualizado no site original, por meio do link: https://journals.lww.com/asaiojournal/Fulltext/2017/11000/Esperanza___The_First_Neonatal_ECMO_Patient.22.aspx
Esperanza: The First Neonatal ECMO Patient
Prolonged extracorporeal circulation for acute heart and lung failure is a technology known as extracorporeal life support (ECLS or extracorporeal membrane oxygenation [ECMO]). Extracorporeal membrane oxygenation is a standard procedure in advanced neonatal pediatric and adult intensive care units (ICUs) around the world. It was not always so.
The first successful prolonged extracorporeal circulation case was reported in 1972.1 The patient was a young trauma patient who was dying from adult respiratory distress syndrome (ARDS), which was a new term defining severe respiratory failure.2 Several more cases followed, and it looked like ECLS would be the answer to what seemed to be (in 1974) an epidemic of ARDS. The Lung Division of National Institutes of Health (NIH) sponsored a multicenter prospective randomized trial of ECLS for ARDS. Only 10% of both the ECMO and the control patients survived, and the study was terminated for futility.3 That study was premature and very poorly designed (by the investigators, including myself)4 and stopped the development of ECMO for adult patients for the next 20 years.
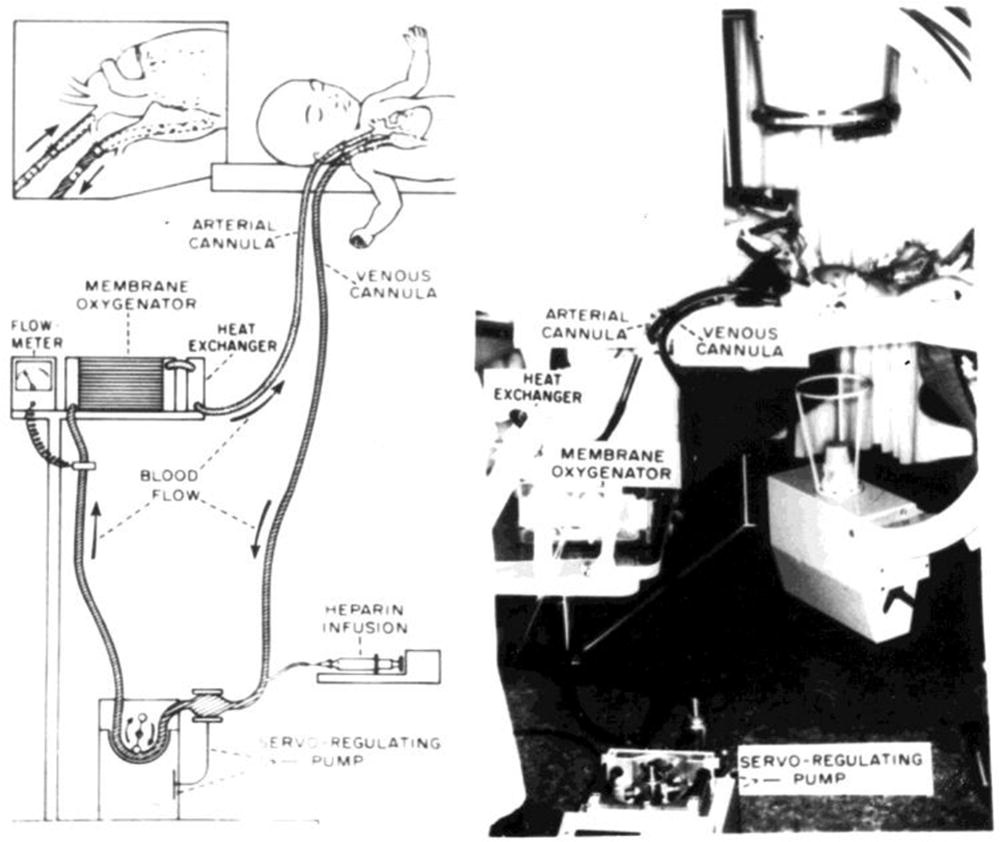
One of the nine centers in the NIH/ECMO study was at University of California Irvine, where we had been developing prolonged extracorporeal support in the laboratory.5,6 We had treated the first successful cardiac support patient in 1972 in a 2 year old child.7 In 1975, we successfully used prolonged extracorporeal support for a newborn infant with severe respiratory failure (Figure 1). At the time, we thought the single case was worth reporting to demonstrate the feasibility and technology of ECMO in neonatal respiratory failure. Journal editors disagreed, and the report was never published. We did report a brief summary of the case in a publication on ECMO in infancy in 1986.8

Looking back, that case turned out to be important because it led to the study and growth of extracorporeal support in newborn infants over the next 20 years. Based on the neonatal experience, ECMO was reactivated in adult respiratory failure and cardiac failure, leading to the widespread practice of ECMO in all age groups for both cardiac and respiratory failure, which is the state of the art today.9
Now, 43 years after that case, we thought it would be interesting to examine that original case report to determine what we had learned at that time and how that case has influenced the growth of ECMO since then. The original case report, written in May 1976, follows:
Extracorporeal Membrane Oxygenation (ECMO) for Newborn Persistent Fetal Circulation
Robert H. Bartlett, Alan B. Gazzaniga, Susie W. Fong, Houchang D. Mondanlou, Claude B. Oliver, Donald R. Sperling
A full-term newborn girl with severe hypoxia and cyanosis was treated with venoarterial cardiopulmonary bypass with a membrane oxygenator (ECMO) for life-support. Angiograms demonstrated minimal pulmonary blood flow, a large main pulmonary artery, and a patent ductus arteriosus with a total right-to-left shunt. The ductus was ligated on ECMO and support continued. Pulmonary function gradually changed from minimal gas exchange, high pulmonary vascular resistance to adequate gas exchange, low pulmonary vascular resistance. At seven days of life, the baby was weaned off ECMO and at nine days of life off mechanical ventilation.
This is the first successful case of prolonged total cardiopulmonary support in a newborn. It demonstrates the effectiveness and safety of ECMO and the reversibility of persistent fetal circulation syndrome.
In the fetus, two thirds of venous return is received and ejected by the right ventricle to the pulmonary artery. Only 5–10% of pulmonary flow is distributed to the lungs, and the remainder crosses the ductus arteriosus to the descending arota.21 Pulmonary arterial pressure is equal to or slightly greater than aortic blood pressure during fetal life. At birth, rapid reduction of pulmonary vascular resistance and increase in pulmonary blood flow occurs. The ductus arteriosus constricts in response to a rise in systemic arterial PO2, so that in the normal infant, functional closure occurs within 10–15 hours after birth. If PaO2 is reduced because of primary lung disease or congenital heart disease, the ductus arteriosus may not close.
Sustained elevation of pulmonary vascular resistance, which prevents adequate pulmonary perfusion, has been called “ Persistence of the Fetal Circulation (PFC)”10 and/or persistent pulmonary vascular obstruction.22 The severity ranges from transient cyanosis with rapid improvement to minimal pulmonary flow, hypoxia, and death.
Life support by prolonged extracorporeal membrane oxygenation (ECMO) has been evaluated in the laboratory, and clinically13 in patients with acute pulmonary insufficiency unresponsive to conventional management. Since the first surviving case was reported by Hill et al. in 1972,14 at least 24 more successful cases have been accomplished,11 including four children.5,23,12,16 ECMO support has been attempted in several infants with idiopathic respiratory distress syndrome (IRDS)25,7,15 and meconium aspiration,15 all without success. We recently had the opportunity to treat a newborn with persistent fetal circulation using ECMO support.
Protocol and Methods
Since ECMO has major potential inherent risks, it is currently considered only in moribund patients. Newborn infants are considered for ECMO support when the neonatologist feels there is no significant chance of survival with maximal conventional therapy. If there are no contraindications (signs of neurologic damage, bleeding, or irreparable congenital anomalies) ECMO may be instituted. The protocol includes fully informed parental consent and is approved by the Human Subjects Review Committee.
Flow rate through the ECMO circuit is limited by venous blood access. A single large catheter placed through the right internal jugular vein into the right atrium will usually allow flow rates equal to the total cardiac output when drained by 150 cm. of venous siphon (i.e. to the floor). Arterial perfusion must reach the aortic root, even at low flow rates. The size of the arterial catheter is the factor which determines perfusion pressure in the ECMO circuit. Root perfusion with the largest possible catheter is achieved by retrograde cannulation of the right carotid artery, which is ligated distally after verifying adequate collateral brain circulation. Gas exchange capability is limited by the size and efficiency of the membrane oxygenator. The Lands-Edwards one M2 membrane oxygenator can transfer up to 30 cc/minute of oxygen and CO2 at flow rates up to 500 cc/minute. This device is more than adequate for any newborn perfusion. A servo-regulated roller pump which adjusts to variations in venous return, a heat exchanger to maintain temperature, and an electromagnetic flowmeter complete the extracorporeal circuit. The circuit is primed with crystalloid and albumin (to diminish the fibrinogen binding) which is displaced by fresh blood. The hematocrit, electrolytes, and acid-base status of the blood is modified until normal. This is a critical step in infant perfusion, as the extracorporeal blood volume (500 cc) may be two to four times the infant blood volume. Heparin, 100 units/kg, is given during cannulation and a continuous infusion of dilute heparin is maintained throughout ECMO, the dose regulated to keep the whole blood activated clotting time2 between two and three times baseline.3
When adequate cardiopulmonary bypass is established, FiO2 is decreased to .4 or less, peak inspiratory pressure (PIP) is decreased to 20 cm H2O or less, and ECMO flow rate of 80–100 cc/kg/minute is maintained. The status of lung function is evaluated daily by temporarily discontinuing ECMO and measuring arterial and venous blood gases under standard conditions (FiO2 1.0, ventilator pressure 25/2). If lung function improves, ECMO flow rate is gradually decreased at FiO2 .4 and PIP under 20 until ECMO is no longer required (lung function is adequate at those setting).
Case Report
A full term (3370 gm) baby girl was born to a 29-year old gravida 7, para 6, Mexican mother on April 29, 1975, following an apparently uneventful pregnancy and delivery. The baby was cyanotic from the time of birth. Apgar score was 6 and 7 at one and three minutes.
An umbilical artery catheter was positioned at the second lumbar vertebra for monitoring. PaO2 was never over 43 mm Hg despite progressively increasing FiO2, intubation, and mechanical ventilation. Eight hours after birth, at FiO2 1.0, rate 28, tidal volume 35 cc, pressure 23/2, arterial blood gases were pO2 23 mm Hg, pCO2 52 mm Hg, pH 7.23. Peripheral perfusion, arterial blood pressure and urine output were normal. Chest x-ray showed a small pneumomediastinum, and enlarged globular heart, and avascular lung fields without significant pulmonary infiltrates (Figure 1). Electrocardiogram showed right ventricular hypertrophy.

Twelve hours after birth the arterial pO2 was consistently less than 25 mm Hg on an FiO2 of 1.0 with ventilator pressures of 30/5. Despite a minute volume of 10 ml/kg/minute, the PaCO2 was 45 and the pH 7.25. Over the next six hours, gas exchange did not improve despite larger volumes, manual ventilation with 100% oxygen, epinephrine, and bicarbonate. By 18 hours of life the baby was deeply cyanotic with episodes of bradycardia and hypotension occurring with increasing frequency. It was the opinion of the neonatologist (HM) that the child had no significant chance of survival with continuing maximal therapy. Venoarterial bypass was begun 20 hours after birth. At the time bypass was begun, arterial pO2 was 17 mm Hg, pCO2 51 mm Hg, pH 7.29.
The right carotid artery was cannulated proximally with a #12 French polyvinyl catheter (Figure 2), and the right jugular vein was cannulated with a #14 catheter with multiple side holes. Blood flow of 300 u/minute was calculated preoperatively to represent 80% of the cardiac output and was sufficient to maintain total gas exchange.
The enlarged heart and clear avascular lung fields seen on chest x-ray suggested either persistent fetal circulation or a cardiac malformation with right ventricular outflow tract obstruction. Cardiac catheterization and angiography were carried out through the catheters which had been placed for ECMO, using a portable fluoroscope with television tape recording. Injection of dye into the carotid perfusion catheter demonstrated a normal aortic arch with no left-to-right ductus flow, ruling out hypoplastic left ventricle and transposition. Dye injected into the right atrium promptly filled the left atrium, left ventricle, and aorta, proving a right-to-left shunt at the atrial level. The right ventricle also filled on this injection taken in the AP plane, but the right ventricular anatomy could not be precisely defined. Since we had already given 3 cc/kg of contract medium (Renografin™60) and the infant was stable on ECMO support, we decided to wait for excretion of contrast material before continuing the study.
Upon continuing the study the following day, venous catheters passed from the umbilical or femoral vein invariably went through the right atrium into the left atrium and demonstrated at least two normal pulmonary veins. However, the catheter could not be maneuvered into the right ventricle, due in part to the large ECMO catheter which filled the right atrium. Dye injection into the right atrium in the lateral position demonstrated a large right ventricle, normal tricuspid valve, and a large right ventricular outflow tract. Because some of the dye simultaneously went via the patent foramen through the left side of the heart into the aorta, the presence of a ductus with right-to-left flow could not be proven. The presence of normal pulmonary veins combined with the absence of any pulmonary arterial flow on several dye studies suggested that pulmonary artery atresia or persistent fetal circulation was the most likely diagnosis. Further evidence was gained by testing off ECMO. Mixed venous blood from the right atrium and arterial blood from the distal aorta had the same blood gas composition, documenting the absence of pulmonary blood flow. During 3–4 minutes of off-bypass testing, cyanosis progressively deepened as the pO2 fell, leading to bradycardia and brief seizures with divergent gaze, all of which returned immediately to normal with resumed bypass flow. Despite the risks of a thoracotomy in a fully heparinized patient, we felt that a systemic-pulmonary shunt procedure offered the only chance of survival (Figure 3).
At thoracotomy a large pulmonary artery was found which appeared to be normal as far as it could be followed into the lung. A large patent ductus, nearly three times the size of the aorta, was present, through which blood was flowing freely from the pulmonary artery to the aorta. The lung itself was white and firm but did expand with ventilation. The lung itself appeared hypoplastic, as might be seen with association with a diaphragmatic hernia. A lung biopsy was done. With the diagnosis of persistent fetal circulation secured, we ligated the large patent ductus with two objectives in mind; 1) with the ductus ligated pulmonary artery pressure would be able to rise higher than systemic pressure, possibly permitting some lung perfusion, and 2) if the lungs improved and pulmonary vascular resistance fell, the ductus was so large that an extensive left-to-right shunt would certainly develop. The ductus was ligated without difficulty. Pulmonary artery pressure (measured by a catheter placed at operation) rose abruptly to 200 mmHg and there was no evidence of lung blood flow on direct observation. Of course, this would have been rapidly fatal if the infant were not on venoarterial bypass.
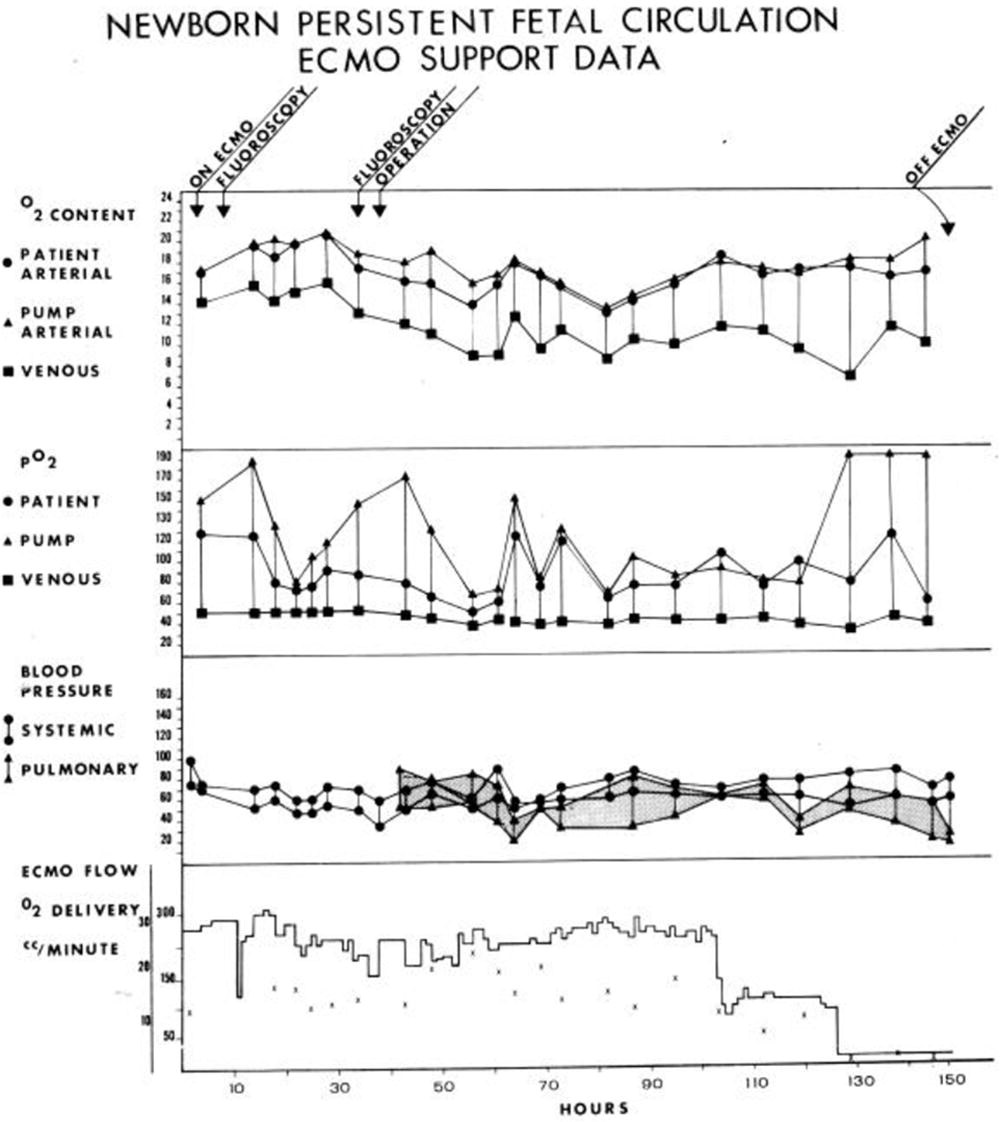
After the operation, the baby was maintained on ECMO. During brief test periods off bypass pulmonary artery pressure rose abruptly, systemic pressure fell, and no gas exchange occurred across the lung (Figure 4). Thirty-six hours after operation, a difference was noted between arterial and venous pCO2 and the pO2 during off bypass testing, although pulmonary artery pressure remained high. Pulmonary function gradually increased so that three days after operation the arterial pO2 off bypass reached 130 at FiO2 1.0. Pulmonary artery pressure was equal to systemic at this point. As lung function improved, ECMO flow was gradually decreased and finally maintained at 50 cc/minute for 12 hours with adequate gas exchange. The baby was alert and responsive during the ECMO course.

Changes in coagulation, platelets, and platelet function in this patient are shown in Figure 5. Throughout ECMO fibrinogen remained at 100–200 mg%, Factor VIII 100–150%, Factor V 50–70%. Screening tests (PTT, PT, and TT) reflected these values. Fibrin degradation produces (FDP) remained at 20–60 mg/ml, except following one episode of low heparin dose on the fourth day when FDP increased to 150 mg/ml associated with a transient drop in fibrinogen and Factor VIII. Platelet count decreased slowly from 80,000 to 30,000, but could be increased with platelet transfusions. Platelet adhesiveness was normal (40–80%) throughout, but ADP aggregation was prolonged and platelet Factor III activity was decreased. All coagulation and platelet parameters returned to normal one week after ECMO.

The catheters were removed and the vessels ligated at 7 days of life, after 6 days of ECMO. Mechanical ventilation was continued, and FiO2 gradually weaned down over the next 36 hours. PEEP was decreased gradually and the baby was extubated at 9 days of life. Pulmonary artery pressure continued to fall during this time and was 30/15 with a systemic pressure of 80/65 when the PA catheter was removed on the tenth day of life.
Chest x-rays showed a progression from small, fully aerated lungs with no blood flow t slight bronchovascular markings, to the ground glass appearance and air bronchograms typical of IRDS, to clearing and progression to normal appearance (see Figure 1). Lung physiology improved as the x-ray pattern appeared to be deteriorating and improvement by x-ray lagged several days behind the physiologic status.
No further cardiopulmonary problems occurred during hospitalization. As the baby grew, spasticity of the right arm and incoordinated swallowing became obvious, although perception and responsiveness appeared normal. Gavage feeding was carried out for two months. Neurologic function slowly improved, and the child was eating normally at discharge 10 weeks after birth. Right arm spasticity had decreased. At 12 months of age, the child has a normal growth curve in the tenth percentile and normal psychomotor function.
Discussion
Clinical ECMO support in the newborn was carried out by Dorson et al. (6 cases),7 White et al. (3 cases),25 and Pyle et al (2 cases),15 and ourselves (2 cases prior to this patient). Although the perfusions were technically satisfactory, all patients died, primarily related to bleeding and neurologic problems. Clinical application of ECMO has focused on older children and adults with reversible pulmonary insufficiency. This technique has been used in over 250 patients for 24 hours to 3 weeks.11 The physiologic and hematologic responses to prolonged ECC have been characterized in the laboratory8 and clinically.5 With this understanding has come smoother, simpler, uncomplicated prolonged perfusion, heparin titration, and control of bleeding.
ECMO flow is begun at a slow rate until the entire prime is thoroughly mixed in. Bypass flow is gradually increased until approximately 80% of the venous return is directed through the extracorporeal circuit. This is the point at which the pulmonary artery and systemic pulse contour become nonpulsatile during ventilator inflation, hence, is easily identified.5 Eighty percent bypass is sufficient to sustain total gas exchange if necessary. Once the desired ECMO is achieved, the patient is monitored and cared for by one nurse and the ECMO system by one technician. Blood is infused to maintain the desired ECMO flow and systemic blood pressure.
Because the heparin effect is dependent on platelet numbers and function as well as protein coagulation factors, it is essential to follow heparin effect with whole blood ACT measurements rather than measurements on plasma.
Hematologic and coagulation changes during prolonged ECMO have been characterized in the laboratory and patients.13,16,26,8 Patients who enter ECMO with established consumption coagulopathy (as was the case with this patient) usually improve during perfusion. Progressive thrombocytopenia and platelet dysfunction is the major side effect. This patient required a major thoracotomy while fully heparinized on ECMO. To facilitate this operation, platelets were infused immediately prior to operation and cautery was used liberally. Minimal bleeding occurred throughout the procedure. Postoperatively continuously oozing occurred at the rate of approximately 300 cc/day. This gradually decreased with time and more platelet transfusion, and essentially stopped after 48 hours.
The syndrome of persistent fetal circulation was recognized by Avery,1 Robertson,20 and Gatti,9 and finally documented by Gersony et al.,10 in 1969. Four of five patients reported Siassi22 with this syndrome survived but two additional cases reported by Gersony et al.,10 were fatal despite attempted therapy with Priscoline™ in one case. Two cases were treated by Burnell et al.,6 had sustained pulmonary hypertension and right-to-left ductus shunts which reversed with oxygen breathing. Both patients died in the third month of life. One case reported by Levin et al.17 did not have life-threatening hypoxemia, but did have elevated pulmonary vascular resistance and right-to-left ductus shunt 2 ½ months after birth, with angiographic small vessel changes persistently to age 22 months. Nielsen et al. identified 16 cases in a newborn ICU, with 38% mortality.19 This syndrome may present any degree of severity ranging from near total absence of pulmonary blood flow (with atrial and ductal right-to-left shunting severe enough to cause CO2 retention), to mild elevation of pulmonary pressure seen with tachypnea and cyanosis, as seen in some of Siassi’s patients. Treatment consists of mechanical ventilation and elevated inspired oxygen. Nielsen emphasized role of left ventricular failure, and suggested pressor drugs to support the heart and improve pulmonary flow.
Direct infusion of short-acting vasodilator drugs into the pulmonary artery may decrease pulmonary vascular resistance and improve pulmonary blood flow and oxygenation. Priscoline™ and similar agents have been used with fair success in mild to moderate PFC,10 poor results in severe types such as this patient. Vasodilators were not used in this case.
Lung biopsy showed thickening alveoli and some hyaline membranes typical of moderate RDS. Pulmonary arteriolar hyperplasia was not pronounced.
The conditions which constitute an indication for ECMO support in the newborn will become apparent as more infants are treated. A correlation between alveoloarterial gradient, time, and mortality can be clearly outlined for adults with respiratory insufficiency.4 Similar mortality prediction indices have been developed for infants with respiratory distress syndrome.24 The development of a pulmonary insufficiency index for newborns will help to define indications for ECMO in persistent fetal circulation, IRDS, and meconium aspiration.
Acknowledgements
Many individuals contributed significantly to the development of our ECMO team and to the successful management of this child. These include Doctors Huxtable, John German, Ragner Amlie, John Renner, ECMO laboratory Director H. Vernon Roohk Phd, ECMO technologists Nick Haiduc, Paul Mullin, Tamar Medley, Nancy Wetmore, Claudia Kincy, Susan Dart, Kathy Hagins, coagulation technicians Christine Woldanski, Eleanor Hung, and David Styler. Our special thanks go to anesthetist Rose Wright CRNA, and the outstanding nurses of the neonatal and pediatric intensive care units, Orange County Medical Center.
References
1. Avery ME, Baghdassarian-Gatewood O, Brumley G: Transient tachypnea of the Newborn. Am J Dis Child 111(4): 38–385, 1966.
2. Baden JP, Sonnefield M, Ferlic RM, et al: The BaSon test. A rapid bedside test for control for heparin therapy. Surg Forum 31: 172–174, 1971.
3. Bartlett RH, Isherwood J, Moss RA, et al: A toroidal flow membrane oxygenator: four day partial bypass in dogs. Surg Forum 20: 152153, 1969.
4. Bartlett RH, Gazzaniga AB, Wilson AF, et al: Mortality prediction in adult respiratory insufficiency. Chest 67: 680–684, 1975.
5. Bartlett RH, Gazzaniga AB, Fong SW, et al: Prolonged extracorporeal cardiopulmonary support in man. J Thorac Cardiovasc Surg 68(6): 918–932, 1974.
6. Burnell RH, Joseph MC, Lees MH: Progressive pulmonary hypertension in newborn infants. A report of two cases with no identifiable respiratory or cardiac disease. Am J Dis Child 123: 167–170, 1972.
7. Dorson W, Baker E, Cohen ML, et al: A perfusion system for infants. Trans Am Soc Artif Intern Organs 15: 155–160, 1969.
8. Fong SW, Burns NE, Williams G, et al: Changes in coagulation and platelet function during prolonged extracorporeal circulation in sheep and man. Trans Soc Artif Intern Organs 20A: 239–247, 1974
9. Gatti RA, Muster AJ, Cole RB, et al: Neonatal polycythemia with transient cyanosis and cardiorespiratory abnormalities. J Pediatr 69: 1063–1072, 1966
10. Gersony WM, Duc GV, Sinclair JC: “PFC” syndrome (persistence of the fetal circulation). Circulation 40(suppl 3): 87, 1969
11. Gille JP: Respiratory support by extracorporeal circulation. Bull Physiopathol Respir 10: 373–410, 1974.
12. Hicks RE, Kinney Tr, Raphaely RC, et al: Successful treatment of varicella pneumonia in a leukemic child with prolonged extracorporeal membrane oxygenation. J Thorac Cardiovasc Surg 73(2): 297–302, 1977.
13. Hill JD, de Leval MR, Fallat RJ, et al: Acute respiratory insufficiency treatment with prolonged extracorporeal oxygenation. J Thorac Cardiovasc Surg 64: 551–562, 1972.
14. Hill JD, O’Brien TG, Murray JJ, et al: Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock-lung syndrome). N Engl J Med 286(12): 629–634, 1972.
15. Hunt CE, Pyle RB, Niel WA, et al: Membrane oxygenator treatment of severe neonatal respiratory insufficiency. Pediatr Research 9(4): 397, 1975.
16. Kolobow T, Stool EW, Sacks KL, et al: Acute respiratory failure. Survival following ten days’ support with a membrane lung. J Thorac Cardiovasc Surg 69(6): 947–953, 1975.
17. Levin DL, Cates L, Newfield EA, et al: Persistence of the fetal cardiopulmonary circulatory pathway. Survival of an infant after a prolonged course. Pediatrics 56(1): 58–64, 1975.
18. Mielke CH Jr, de Leval M, Hill JD, et al: Drug influence on platelet loss during extracorporeal circulation. J Thorac Cardiovasc Surg 66: 845–854, 1973.
19. Neilsen HC, Riemenschneider TA: Severe heart failure and cyanosis of the newborn. The persistent transitional circulation syndrome. Presented at AAP-Cardiol Section 44th Annual Meeting, Washington DC, 1975.
20. Robertson NR, Hallidie-Smith KA, Davis JA: Severe respiratory distress syndrome mimicking cyanotic heart disease in term babies. Lancet 2: 1108–1110, 1967.
21. Rudolph AM: Congenital diseases of the heart. Yearbook Medical Publications, Chicago, 1974.
22. Siassi B, Goldberg SJ, Emmanouilides CC, et al: Persistent pulmonary vascular obstruction in newborn infants. J Pediatric 78(4): 610–615, 2971.
23. Soeter JR, Mamiya RT, Sprague AY, et al: Prolonged extracorporeal oxygenation for cardiorespiratory failure after tetralogy correction. J Thorac Cardiovasc Surg 66(2):214–218, 1973.
24. Stahlman MT, Battersby EJ, Shepard FM, et al: Prognosis in hyaline-membrane disease. Use of a linear-discriminant. N Engl J Med 276(6):303–309, 1967.
25. White JJ, Andrews HG, Risemberg H, et al: Prolonged respiratory support in newborn infants with a membrane oxygenator. Surgery 70(2): 288–296, 1971.
26. Zapol WM, Bloom S, Carvalho A, et al: Improved platelet economy using filler free silicone rubber in long term membrane lung perfusion. Am Soc Artif Intern Organs 21:587–592, 1975.
Discussion
Looking back on this case report after 40 years, much of the basic information on ECMO devices and technology has persisted since that time.
Terminology
ECMO appears in the title of this case report. The use of the term ECMO to describe prolonged extracorporeal circulation using a membrane oxygenator was coined in the meetings of the NIH-sponsored ECLS trial. In those meetings, it became convenient to refer to the technology as membrane oxygenation, which does not really describe what prolonged ECLS is all about. However, it was easy to say and became the jargon for prolonged mechanical support during those meetings. The term grew into general usage. Our publication in 19768 was among the first official uses of the term ECMO, which has persisted to this day. The NIH ARDS Trial Group (Extracorporeal Support for Respiratory Failure) was first convened in 1974, and patients were entered into the trial beginning in late 1975. Most of the investigators in that trial and other ECLS investigators from throughout the world met in Copenhagen in 1975 to discuss the possibilities of prolonged extracorporeal support.10 At that meeting, Phil Drinker and I discussed our research over the past 10 years, and I mentioned the successful newborn case.
Authors
The University of California Irvine Medical School was opened in 1970. Clinical activity was based in local private hospitals and Orange County Medical Center, a 600 bed general hospital largely serving the barrio population. The chair of surgery was John Connolly who recruited faculty with very broad interests and certification in surgery. Al Gazzaniga and I were recent graduates of the surgical residency at Peter Bent Brigham Hospital and Children’s Hospital in Boston. As the young guys, we were assigned the job of running the surgery program at Orange County Medical Center. Our surgical practice included general, cardiac, thoracic, vascular, trauma, burns, critical care, and pediatric surgery. We took over an abandoned building to establish a large animal research lab devoted to cardiopulmonary physiology and artificial organs. In that lab, we developed a team of nurses and perfusionists to study prolonged extracorporeal circulation. This was supported (since 1971) by an NIH grant, which continues today. We joined with collaborators, hematologist Susie Fong and cardiologist Don Sperling. Because we were the pediatric surgeons, it was not unusual for neonatologist Houchang Modanlu to ask our opinion about a puzzling baby with respiratory failure. Claude Oliver was a resident in cardiothoracic surgery.
In retrospect, much of ECMO development (and much of critical care) grew out of the opportunity to manage neonates, children, and adults in the OR and ICUs every day.
Introduction to the Case Report
The introduction in this article summarizes the previous cases reported in all age groups. Very few successful cases existed at the time. Under the Methods section, the technique, devices, and protocols for ECMO management are discussed as if it was a routine practice. In fact, our approach had been in development since 1965.11,12 We had described modified roller pumps for prolonged support and the technique of titrating heparin to a measured clotting time. At the time, there were a few membrane oxygenators available for prolonged support. We were using the Lande–Edwards oxygenator because it was manufactured at the Edwards laboratories, which was a few miles from our hospital. Don Hill had used the Bramson oxygenator which was custom made on site for each case.13 Ted Kolobow was beginning laboratory studies on the spiral coil oxygenator, which later became the standard device for the next 25 years.14
Indications
The indication for attempting ECMO in a newborn (or any patient at the time) was based on the clinical judgment of the attending physicians. If a patient’s condition was judged to be fatal respiratory failure, ECMO was considered in the very few centers that had that technology under study in the laboratory. In this case, the neonatologists at University of California, Irvine, Dr. Modanlu and Dr. Robert Huxtable, agreed that the child would die with continuing conventional care. That care is described in some detail in the report. Many years later, we developed the neonatal oxygenation index to define the severity of respiratory failure in newborn infants.15 The oxygenation index is calculated as the mean airway pressure times the fraction of inspired oxygen divided by the arterial PO2. An oxygenation index of 20 indicates about 50% mortality risk, and an oxygenation index of 40 carries 80% mortality risk. This has become standard practice in neonatology for many years. Calculating the oxygenation index in this patient, it would have been 147 (mean airway pressure 25 × 100% oxygen ÷ 17).
Vascular Access
As in our previous infant cases, we used direct access via the right carotid and jugular. This approach at the time seemed dangerous and in fact seems dangerous today, ligating these major head vessels in newborn infants. We knew that this technique would be safe because of our extensive laboratory experience demonstrating ample collateral through the face and the pharynx to the brain when one common carotid artery is ligated. Surgeons had used the left carotid on occasion for a Blalock Taussig shunt without complications when the subclavian was not available. Nonetheless, this approach to extrathoracic vascular access was considered outrageous at the time. Over the years, it has become standard practice for venoarterial access in infants.
ECMO Management
The basic approach to ECMO management described in the Introduction was used successfully during this case. Venoarterial perfusion at 80–100 cc/kg/min provided both cardiac and respiratory support. This allowed time for evaluation and diagnosis and time for recovery of normal cardiopulmonary function. Lung function was assessed during brief periods off bypass, and ECMO was gradually weaned when lung function improved.
An unusual aspect of the case is the dilemma in diagnosis and the fact that we simply went to the operating room to take a look and determine what the problem was. This may seem a little cavalier, but it was not unusual for us (Robert E. Gross trained surgeons) to simply consider direct access as a step in the algorithm of diagnosis and management. We did find a huge patent ductus arteriosus, but the blood was flowing right to left. We ligated the ductus, and the right ventricle promptly distended. The child would have died on the spot if she were not on venoarterial bypass. However, we did not see an anatomic reason for the profound right ventricular distension, so we put a catheter into the main pulmonary artery (PA) and measured the pressure. The PA pressure was supra systemic, although we did not see any abnormalities in the lungs themselves. At the time, I thought we were dealing with an unusual pulmonary arteriolar abnormality, which would be fatal. However, I did not want to terminate ECMO in the operating room, so we returned to the neonatal ICU. The next day, when I planned to terminate the procedure for an incurable congenital anomaly, the PA pressure dropped, CO2 excretion occurred, and the patient began to improve. In retrospect, the pulmonary vasospasm relaxed, and normal cardiopulmonary anatomy and function was demonstrated. As noted in the report, we periodically turned off ECMO and measured pulmonary function. Initially, there was none, but as pulmonary blood flow returned, native lung function also returned, and we could wean off extracorporeal support on ECMO day 6. Ventilator support continued for several days, and then the patient remained in the neonatal ICU for almost 3 months. This long neonatal hospitalization was not unusual at the time. First of all, she had no home to go to (discussed later). Second, she was having some right-sided weakness and trouble swallowing, which required a long workup and management plan. (The patient ultimately had no neurologic disability.)
Anticoagulation
All the investigators developing this new technology used heparin as the anticoagulant because that is what we used in the operating room for cardiac surgery. It provided quick and effective total anticoagulation and could be reversed at the end of a cardiac operation. Using heparin for prolonged extracorporeal circulation always led to bleeding in the early development, so we developed the technique of titrating heparin to the very lowest level that would provide a little anticoagulation without causing bleeding.11 To do this, we had to have a simple method of measuring the effective anticoagulation. It was important to do this in whole blood rather than just plasma. We modified the technique of Bader and Sonnenfield in which a stimulus was added to a Lee-White clotting time device and the time it took the blood to clot was measured.16 For the stimulant, we initially used the same reagent used for the partial thromboplastin time (rabbit brain thromboplastin) and used this for many years early in the development of ECMO. Ultimately, it proved to be simpler to use kaolin, and companies developed devices to automatically measure the time it took the blood to clot. Titration of intravenous infusion of heparin is still the standard method of managing anticoagulation during ECMO, but it has become more rather than less complicated as a variety of serious hematology researchers point out that there are other ways of measuring the amount of heparin in the blood. Currently, measuring anti-Xa is commonly used. However, we are not interested in the amount of heparin in the blood only in the heparin effect. In fact, the heparin effect in whole blood is what we really need to know. Therefore, the old-fashioned activated clotting time or the new-fashioned thromboelastogram is the best way to monitor anticoagulation during ECMO. With new devices that have been available for the last decade, it is possible to manage a patient on ECMO for days or weeks at a time without systemic anticoagulation.
Diagnosis
The diagnosis listed in the title and the case description is newborn-persistent fetal circulation. We came to that diagnosis several days into the course managing this patient. Much of the case report describes the diagnostic dilemma. There had been some meconium aspiration, but neither the clinical course nor the chest x-rays looked like severe meconium aspiration. In fact, the lung fields were remarkably clear showing very little pulmonary vasculature. We initially considered the problem to be congenital heart disease and undertook a series of studies to evaluate the anatomy of the heart. Modern day readers may not recognize that echocardiography was not available. Cardiac catheterization was possible, but the patient was already on venoarterial bypass with a large catheter (made from a chest tube) filling the right atrium, so we were unsuccessful at cardiac cath. Rather, we conducted two series of cineangiograms through the existing ECMO catheters to try to determine the cardiac and vascular anatomy. We could not establish a definitive diagnosis, although it was clear that right atrial injection appeared on the systemic circulation very quickly. A few cases of fetal circulation persisting beyond birth had been reported in the literature but persistence of the fetal circulation as a definitive diagnosis had never been established. When it was clear that persistent pulmonary hypertensive was in fact the correct diagnosis, we went on a more serious literature search and found scattered cases which were usually fatal. The original description was by Walter Gersony in 1969. Walter Gersony was a cardiology fellow at the Boston Children’s Hospital when we were surgical residents at the same hospital. Partly because of this case, we began to look for persistent pulmonary hypertension and fetal circulation in other cases and discovered that the basic pathophysiology of most neonatal respiratory failure was characterized by pulmonary arteriolar spasm and right to left shunting. As this became recognized, the concept of inducing alkalosis by hyperventilation sometimes resulted in relaxation of the pulmonary vasospasm and that became standard practice when persistence of the fetal circulation was suspected. In retrospect, that hyperventilation caused much more primary lung injury than it improved patient care. By the early 1990s, the role of inhaled nitric oxide to relax the pulmonary vasospasm was recognized and became standard practice. Inhaled nitric oxide is even more efficient in the newborn when used with high frequency oscillation. By the mid-1990s, the primary diagnosis of persistent fetal circulation syndrome persisted, but ECMO was almost never necessary in the management. We could use the term persistent fetal circulation with confidence because we had the unusual situation of having placed a PA catheter, demonstrating supra systemic PA pressures, which resolved over a few days.
Follow-Up
In 1985, I was scheduled to give the presidential address at the American Society for Artificial Internal Organs. Taking advantage of that opportunity to present this case report, I titled the address “Esperanza.”17 I explained that this child was an orphan and named by the nurses Esperanza, which means hope in Spanish. Most of the ECMO community knows about that address and publication, and Esperanza herself is a celebrity within the ECMO community. The reason that she was an orphan was that her mother was in the country illegally when she went into labor. It was fairly common practice for poor Mexican mothers to deliver their babies in the United States at that time to bestow the gift of US citizenship. The mother was told that the child would surely die and she gave consent for trying a totally unproven approach, but promptly left the hospital concerned over her legal status. When Esperanza was ready to be discharged, she went to a wonderful foster family who took care of her throughout her development life. She was a healthy child as long as I followed her (for a couple of years), but the family moved away from California, and I lost track of her altogether. In 1989, I received a call from a pediatrician in Missouri who said he had a most unusual young girl in his office. She had some minor complaints but had unusual scars on her right neck and her left chest, and her chest x-ray showed what seemed to be a section of plastic catheter in her right lower lobe. This was Esperanza! When I had removed the silicone rubber catheter from her PA several days after ECMO, it broke off at the site of entry into the PA, and a segment lodged in her right lower lobe. We thought about trying to retrieve it at the time but it was causing no problems so we simply left it. It is still there today. Because of this call, I made contact with Esperanza. We became friends, and at age 21, she attended one of the early extracorporeal life support organization (ELSO) meetings in 1996 (Figure 2). Since that time, she has become a wife and a mother. Her daughter recently joined the air force. Esperanza and her daughter, Rhonda, attended the 25th anniversary meeting of ELSO in 2015.

Impact
At the time we treated Esperanza, the multicenter NIH trial of ECMO for adult respiratory failure was just beginning. We entered several cases into that trial. The end result was only 10% survival in both treatment and control groups, which essentially stopped research on ECMO for adult respiratory failure for the next 20 years. However, based on the success with Esperanza, we evaluated ECMO in severe newborn respiratory failure over the next several years, with about 50% successful survival.18 In 1980, I moved to the University of Michigan along with the NIH grant supporting the neonatal ECMO research. The neonatologists, Deiter Roloff and Bob Schumacher, were appropriately skeptical but joined into the project and became invaluable collaborators. Other neonatologists became interested, and we established courses in neonatal ECMO. By the time there were several centers, we established a registry of cases which became the basis for the Extracorporeal Life Support Organization.19 Only a few centers around the world had continued to study ECMO for adult respiratory failure.20–22 The swine flu epidemic of 200823 and the new devices for ECMO which became available in 200924 prompted worldwide interest in ECMO for respiratory failure, and it is now standard practice in most advanced adult ICUs. Application of ECMO for cardiac support has been standard in pediatrics since the 80s25 and has now grown to use in adult cardiac failure26 and in the management of cardiac arrest.27
Conclusion
It is remarkable how little has changed in ECMO since this first successful neonatal case. The physiologic understanding, the concept of resting the lung from ventilator damage, the method of managing the flow rate, the sweep gas flow rate and the native circulation, and the method of anticoagulation are essentially the same now as in 1975. New oxygenators and pumps have greatly improved the safety and simplicity of the circuit. New direct thrombin inhibitor anticoagulants are replacing heparin because of simplicity of management and measurement. Double lumen cannula venovenous access (developed in our laboratory in 1982 by Zwischenberger28) is now the method of choice for pure respiratory failure. Awake management with ambulation and physical therapy has replaced prolonged sedation. The Extracorporeal Life Support Organization now has chapters on five continents and is the worldwide voice for prolonged extracorporeal support. However, it is interesting to look back on the initial successful neonatal case. It has had quite an impact on critical care and medical practice.
References
1. Hill JD, O’Brien TG, Murray JJ, et al. Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock-lung syndrome). Use of the Bramson membrane lung. N Engl J Med 1972.286: 629–634.
2. Ashbaugh DG, Petty TL. Sepsis complicating the acute respiratory distress syndrome. Surg Gynecol Obstet 1972.135: 865–869.
3. Zapol WM, Snider MT, Hill JD, et al. Extracorporeal membrane oxygenation in severe acute respiratory failure. A randomized prospective study. JAMA 1979.242: 2193–2196.
4. Spinelli E, Bartlett RH. Relationship between hemoglobin concentration and extracorporeal blood flow as determinants of oxygen delivery during venovenous extracorporeal membrane oxygenation: a mathematical model. ASAIO J 2014.60: 688–693.
5. Fong SW, Burns NE, Williams G, Woldanski C, Gazzaniga AB, Bartlett RH. Changes in coagulation and platelet function during prolonged extracorporeal circulation (ECC) in sheep and man. Trans Am Soc Artif Intern Organs 1974.20A: 239–247.
6. Bartlett RH, Fong SW, Burns NE, Gazzaniga AB. Prolonged partial venoarterial bypass: physiologic, biochemical, and hematologic responses. Ann Surg 1974.180: 850–856.
7. Bartlett RH, Gazzaniga AB, Fong SW, Burns NE. Prolonged extracorporeal cardiopulmonary support in man. J Thorac Cardiovasc Surg 1974.68: 918–932.
8. Bartlett RH, Gazzaniga AB, Jefferies MR, Huxtable RF, Haiduc NJ, Fong SW. Extracorporeal membrane oxygenation (ECMO) cardiopulmonary support in infancy. Trans Am Soc Artif Intern Organs 22: 80–93–1976, .
9. Thiagarajan RR, Barbaro RP, Rycus PT, et al. Extracorporeal Life Support Organization International report 2016. ASAIO J 63:60–67–2017, .
10. Zapol WM, Qvist J. Artificial Lungs for Acute Respiratory Failure. 1976.New York, Academic Press.
11. Bartlett RH, Kittredge D, Noyes BS Jr, Willard RH 3rd, Drinker PA. Development of a membrane oxygenator: overcoming blood diffusiolimitation. J Thorac Cardiovasc Surg 1969.58: 795–800.
12. Bartlett RH, Isherwood J, Moss RA, Olszewski WL, Polet H, Drinker PA. A toroidal flow membrane oxygenator: four day partial bypass in dogs. Surg Forum 1969.20: 152–153.
13. Bramson ML, Osborn JJ, Main FB, O’Brien MF, Wright JS, Gerbode F. A new disposable membrane oxygenator with integral heat exchange. J Thorac Cardiovasc Surg 1965.50: 391–400.
14. Kolobow T, Bowman RL. Construction and evaluation of an alveolar membrane artificial heart-lung. Trans Am Soc Artif Intern Organs 1963.9: 238–243.
15. Heiss KF, Bartlett RH. Extracorporeal membrane oxygenation: an experimental protocol becomes a clinical service. Adv Pediatr 1989.36: 117–135.
16. Baden JP, Sonnenfield M, Ferlic RM, Sellers RD. The BaSon test: a rapid bedside test for control of heparin therapy. Surg Forum 1971.22: 172–174.
17. Bartlett RH. Esperanza. Presidential address. Trans Am Soc Artif Intern Organs 1985.31: 723–726.
18. Bartlett RH, Andrews AF, Toomasian JM, Haiduc NJ, Gazzaniga AB. Extracorporeal membrane oxygenation (ECMO) for newborn respiratory failure: forty-five cases. Surgery 1982.92:425–433.
19. Toomasian JM, Snedecor SM, Cornell R, et al. National experience with extracorporeal membrane oxygenation (ECMO) for newborn respiratory failure: Data from 715 cases. ASAIO Trans 1988.34:140–147.
20. Kolla S, Awad SS, Rich PB, Schreiner RJ, Hirschl RB, Bartlett RH. Extracorporeal life support for 100 adult patients with severe respiratory failure. Ann Surg 1997.226: 544–564; discussion 565.
21. Pesenti A, Gattinoni L, Kolobow T, et al. Extracorporeal circulation in adult respiratory failure. ASAIO Trans 1988.34:43–47.
22. Lewandowski K, Rossaint R, Pappert D, et al. High survival rate in 122 ARDS patients managed according to a clinical algorithm including extracorporeal membrane oxygenation. Intensive Care Med 1997.23: 819–835.
23. Davies A, Jones D, Bailey M, et al. Extracorporeal membrane oxygenation for 2009 A(H1N1) acute respiratory distress syndrome. JAMA 2009.302:1888–1895.
24. Simons AP, Weerwind PW. Evaluation of Quadrox-i adult hollow fiber oxygenator with integrated arterial filter. J Extra Corpor Technol 2010.42: 242; author reply 243.
25. Kulik TJ, Moler FW, Palmisano JM, et al. Outcome-associated factors in pediatric patients treated with extracorporeal membrane oxygenator after cardiac surgery. Circulation 1996.94(9 suppl): II63–II68.
26. Pagani FD, Lynch W, Swaniker F, et al. Extracorporeal life support to left ventricular assist device bridge to heart transplant: a strategy to optimize survival and resource utilization. Circulation 1999.100(19 suppl): II206–II210.
27. Tonna JE, Johnson NJ, Greenwood J, et al. Practice characteristics of emergency department extracorporeal cardiopulmonary resuscitation (eCPR) programs in the United States: The current state of the art of emergency department extracorporeal membrane oxygenation (ED ECMO). Resuscitation 2016.107:38–46.
28. Zwischenberger JB, Toomasian JM, Drake K, et al. Total respiratory support with single cannula venovenous ECMO: double lumen continuous flow vs. single lumen tidal flow. ASAIO Trans 1985.31:610–615.
ECMO; newborn respiratory failure; history